
the professional perspective
first: a little background
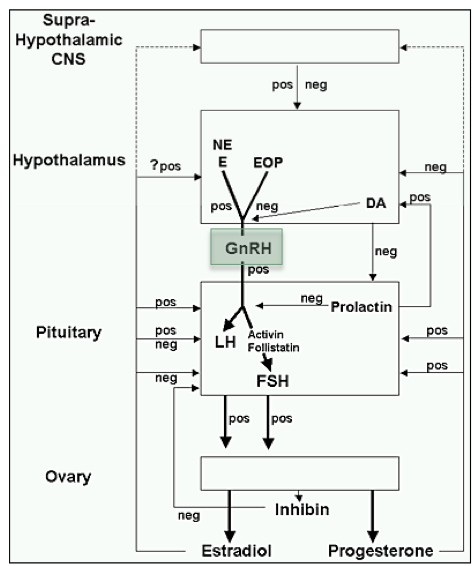 from endotext.org
from endotext.org
okay, don’t freak out! seriously. all i wanted to illustrate with the crazy scheme on that chart is that the controls of reproductive function are complicated. your ovaries aren’t just on autopilot; there are inputs from the brain and the body that are critical for regulation of functions such as ovulation and menstruation.
the hypothalamus is an area of the brain that receives inputs from the rest of the brain as well as hormonal signals from the body [estrogen, leptin, and progesterone — just to name a few of these influences]. to simplify things, depending on what the input signals say, the hypothalamus will either act in favor of or against ovulation [and therefore fertility].
the hypothalamus gets all of this power because pulsatile release of a hormone called GnRH is needed to stimulate the pituitary to make LH and FSH in a pattern that will lead to ovulation. you can see a schematic of this below, or you can just take my word for it.
 GnRH, LH, FSH, and ovarian hormones: on an ideal monthly cycle
GnRH, LH, FSH, and ovarian hormones: on an ideal monthly cycle
if you think about it from an evolutionary perspective, this switch makes absolute sense! if ms. cavewoman was living in less-than-ideal conditions [ie, starvation / very high stress / illness], WHY would she want to pour precious energy and resources into the costly process of ovulation and then reproduction? an undernourished and unhealthy female is unlikely to successfully grow and raise an offspring, so it would be a wasteful endeavor to just let it happen willy-nilly.
some things that the hypothalamus pays attention to
✰ fat stores. via hormones like leptin and estrogen [yes, fat makes estrogen!], the body is able to ‘tell’ the brain what the nutrient situation is like. too little leptin –> a hypothalamus that is not going to be pro-ovulation. this means that BMI may be less important than overall body fat percentage when it comes to fertility [although someone with a BMI of 16 is unlikely to have enough fat to procreate no matter how you slice it].
✰ illness. if a person is chronically ill [poorly-controlled diabetes; inflammatory bowel disease; cancer; lupus; etc], then this can certainly shut things down — another smart evolutionary move. it absolutely does not mean one CANNOT get pregnant while sick, but it does make it less likely.
✰ stress. ‘stress’ is a widely used and very vague term these days. but it’s true: enough of certain types of stress can certainly blunt hypothalamic pulsatility, particularly if one’s hypothalamic axis tends to be on the more sensitive side.
✰ exercise. so that 18 mile long run? it might not have felt like stress to you, but that doesn’t mean the hypothalamus doesn’t view things differently. after all, the primitive brain centers don’t get that you’re just training for fun — they just see a whole lot of very high-intensity activity. were you running from a saber-toothed tiger? or fleeing an unsafe living area? either way, it’s a whole lot of energy expenditure and doesn’t exactly reassure the hypothalamus that it’s baby-making time.
2 months ago, i gave a presentation on HA which focused on a new england journal study recently released; those with journal access and curiosity can see it here. basically, this study aimed to identify genes in patients with what they called functional hypothalamic amenorrhea to find out if there are genetic factors that might underlie susceptibility to this condition.
in other words, they wanted to figure out why some women are more vulnerable to this than others — what makes some hypothalamuses [hypothalami!??] more sensitive than others. ie, how it is possible that victoria beckham has managed to procreate 4 times . . .
 although of course there is no way of knowing what went into these pregnancies and i am not going to speculate!
although of course there is no way of knowing what went into these pregnancies and i am not going to speculate!
in the end, the article DID find some clues as to the genetic basis of hypothalamic amenorrhea — though their findings were just the beginning. however, what i would like to highlight are the criteria these authors used to put someone in the HA category, because in my own experience clinicians and patients are NOT always on the lookout for this condition unless it’s really obvious [ie, 90-lb ballerina with 3 stress fractures].
HA criteria used in the NEJM study
1. Secondary amenorrhea x 6 months or more
2. Low or normal gonadotropin levels [a fancy term for the pituitary hormones LH and FSH]. i’ve heard many people say they don’t think that running or exercise is an issue because their LH and FSH were in the ‘normal range’. i believe that HA is a spectrum, and in some ways it’s the hardest for those who are not at the severe end because it’s not so clear what to do — but normal LH and FSH do not mean a normally-functioning hypothalamic-pituitary-gonadal axis. in this study, the average LH and FSH in the HA group were 4.1 and 6.3 mIU/ml, respectively.
3. Low serum estradiol levels. or low-ISH, really, based on the numbers they provided. unfortunately, the study does not mention how low their specific cutoffs were — and the average value in their HA group was 39 pg/ml. this isn’t a level that would necessarily be called out as ‘abnormal’, but apparently it’s low enough [at least according to NEJM].
4. Normal neuroimaging, no PCOS symptoms/labs
5. One or more predisposing factors below:
Exercise >5 hours/week
History of loss of >15% body weight
Subclinical eating disorder on Eating Attitudes Test
this was not among the criteria, but of note the average BMI for this group was 19.4. ie, on the low end, but not an unhealthy BMI by official standards!
in the end, using the above criteria, the study identified a decent proportion of patients [7 out of 55] with mutations in some of the genes involved in hypothalamic control, while NO mutations were found in a control group of women who had HA risk factors [ie, were exercising > 5 hours/week] but were ovulating normally. this doesn’t mean that we completely understand what may make you more vulnerable to HA than your running partner, but it hints that there’s probably a genetic basis.
ie: to some extent, it’s the luck of the draw.
the personal perspective
i’m not going to rehash my entire TTC saga — it’s here after all [and you all know the happy ending]. but here are some things i WISH i had known during my experience with infertility, which i now believe was at least in part secondary to hypothalamic dysfunction. after all, for over a year and a half i easily met the criteria in this study: i had complete amenorrhea with labs and BMI that fit the above profile almost exactly, and i was exceeding 5 hours/week of exercise on a regular basis. [of note, that may sound like a lot, but even an intermediate half-marathon training plan will often approach that amount, especially if you add in weights/stretching and include less intense exercise in the total.]
✔ this is very common. i often felt like the odd one out with my issues — after all, i was not extremely thin nor a ‘real’ athlete — i was just recreational! however, there is more and more research pointing to evidence for ovulatory dysfunction [both amenorrhea and more subtle phenotypes] in women who exercise more. and an astute reader [and now friend] led me at some point to this hypothalamic amenorrhea message board, which helped me realize that i was not alone. i definitely recommend checking it out if you are in a similar situation.
✔ the world won’t end if you run less! and, you can often still enjoy SOME exercise while bringing things to a level that makes your hypothalamus happy. i found solace in yoga [fun] and a very reduced [but still-present] running load. at one point, i was attending vinyasa classes 2-4 times/week and running 2-3 times/week — 3 miles at a time max. i was never completely inactive, but the changes were apparently enough for my body to respond*
✔ a little weight gain is not the end of the world either — and it might help. actually, to this day i have no idea which factor was more important: the change in my workouts, or the ~8 lbs i purposefully gained [mostly just by not changing my eating much with the reduced activity] to bring my BMI up to around 21. i am not going to lie: it was not fun growing out of some of my own clothes. but in the end it was 100% worth it. i promise.
✔ you may have to take matters into your own hands. this one was very hard for me — after all, i am a medical professional — in the field of endocrinology — so i wanted to trust the experts! i saw a reproductive endocrinologist through all of this who never made a concrete suggestion to me regarding weight and/or exercise, even as i failed to respond to multiple rounds of clomid in a row. i suppose she felt that my activity/weight did not put me in the obvious HA category, and thought i had some other issue, but i believe that the fact that i only started ovulating consistently with after the above changes — even with medication — tells most of my story. given how much of a problem obesity is in our society [and in medicine], i think it is hard for doctors to tell someone with a ‘normal’ BMI to gain weight or cut down on exercise.
after i did finally get pregnant, she made some remark to me that she got pregnant when she was injured and couldn’t run [this physician happens to be quite thin]. umm, not so helpful AFTER THE FACT. i can’t begrudge her too much, because hey — now i’m hanging out at 23 weeks! but i wish i had gotten more feedback on this early on.
* although i did get pregnant while taking letrozole, i did not consistently respond to fertility medications until making the above changes. and i still wonder if i could have done it all-natural — however, at that point my mental state was a mess and i wanted to hurry things up and be proactive as much as i could. i do not regret this one bit!
whew!
okay, i hope that was helpful and not just wayyyyy too much! please note that i am not offering individualized advice in the above — obviously, every case is different! but the above is some background [through the eyes of a pediatric endocrinology fellow] and then my own experiences. feel free to share your own similar or conflicting findings here, or email me if you have questions [although again — obviously, i cannot give out official medical advice!].
——————————————————————————–
12.5.11
workout: tracey mallett pregnancy fitness dvd. cheesy but i sort of like it!
monday classic i could pretend that i turn to amy’s pizza on many mondays because it’s the ONLY convenient option, but the truth is . . . i just kinda like it. it’s comfort food to me at this point!

i took things up a [minor] notch last night and accompanied the usual with a west-coast-themed salad: spinach, tomatoes, avocado, cashews, and raisins, all in a vinaigrette made with a splash of honey.
tonight i’ll christen our new apartment kitchen with its first real home-cooked meal.
spanish: si
reading: check — yes even on call. the pager was pretty quiet, so i took advantage.
20 Comments
LOVE this. I had secondary amenorrhea and didn’t get my period for more than a year (!!!). After many tests, ruling out PCOS, hypothyroidism, etc., I ended up using progesterone challenges to jumpstart things…I also cut way down on my running, started eating more fats and finally, my cycle got back to normal. But I’m terrified about the effect on my fertility, so I appreciate this explanation.
Thanks for putting this together for us. I totally agree with the "take things into your own hands" statement. I had a total breakdown after the first GYN I saw told me- after one failed round of clomid- that the only thing that would work for me was IVF-type reproductive help. I got on my insurance website and found a doctor who actually ordered a pelvic ultrasound to see if there was anything physically wrong and is fine with continuing to try clomid and other less drastic measures before condemning me to never having a child without a $10k medical procedure. Even though I’m not sure I’m ovulating yet, I *feel* much more like I’m making progress, and it’s helped me commit to cutting back on running to 3mi 3x a week + yoga. Sometimes I feel like I’ll never get pregnant, but your story (and some other friends who had reproductive problems) help keep the hope alive!
Wonderful post Sarah
Fantastic post Sarah – love love it. And this post has come at such a perfect time for me because this week has been somewhat hard in the lessening of the exercise and seeing my weight go up – but this post just reaffirms to me that it’s most definitely worth it and you’re proof that with these lifestyle changes, pregnancy will come true. I’m also a member of that board and it would be very hard to go through this without their amazing support – it helps so much to know I’m not alone in this and when I have days where I want to give up and go get that intense workout in, I go to the board and am reminded to stay on the right track and to not give up! Thank you again Sarah for this post – I’m bookmarking it for when I need that extra motivation and inspiration during this difficult time – reading this again and again will keep my chin up and moving forward on this journey.
Great post Sarah! I also wish my doctor encouraged me to cut back on running and gain weight despite my healthy BMI. I still don’t know if I have HA or PCOS, but I guess time will tell as I start prepping my body for the next go around.
Nice little refresher on repro physiology! I actually am oligomenorrheic. However, I am on a pill which only has a 4 day placebo part. I don’t think it gives me enough withdrawal time to bleed. My sports medicine doctor thought I had "female athlete triad," but I don’t think I quite fit that. I did actually experiment and delay the next start by a day and i did get my period (and actually bled through the first week of pills, which is weird.) If its not enough withdrawal time, then I think I prob do have some sort of HA as my loss of periods usually corresponds to high levels of school + running stress. I’m hoping my bone density is ok though, especially since I receive exogenous estrogen from the pill.
Wow! Fantastic post! As someone who has struggled with amenorrhea in the past, it is so helpful to know all the factors that can impact its occurrence. Thanks so much!
Loved this. I’m not TTC but think your whole post is such a good reminder of how many different variables there are on the system. Such a huge balancing act and you explained it well.
Great post. I’m not TTC but I likely will be in a few more years and, having been on BC for the last 7 years and being a marathoner, I’m a little concerned about it. I wish there was a way to know BEFORE TTC if you will have any issues! Hopefully things will go smoothly, but I will likely come back to this post! 🙂
Interesting post! I belive all bodies are different though. For me, I was regular as clock work at a BMI of 19 and a steady mileage of 50+ mpw. Then I developed an inflammatory bowel disease and have to be on immunosuppressants and my reproductive system just shut down. Gaining weight and reducing running did nothing for me. But on the other hand I ovulate easily on clomide. So happy to be sharing this pregnancy experience with you! It took a while, but we both got here evemtually!
Hi. I just wanted to chime in here. I actually came to your blog a few months back via a HA link of some kind (can’t remember what right now). I was initially diagnosed with PCOS (based on ultrasound and lack of menstruation) but didn’t really have the usual hormone profile. And, my BMI was something like 17 or 18, although it always has been, I’m just kind of a rail. Plus I’m very active, kind of type A, you know, the usual HA stuff.
Anyway, I had been TTC for 2+ years, and seeing a fertility specialist… doing the letrozole routine (despite his repeated encouragement to move quickly to IVF). After "failing" my last letrozole cycle, my husband and I conceived spontaneously. When I met with the specialist again, he asked me "why are you pregnant?" I told him that I thought it was because I had gained weight (primarily by eating a lot more protein and meat and carbs fyi). He actually told me that they had always been worried about my BMI, but that "they don’t counsel lifestyle issues". I was floored. Really? It is possible I could have conceived a year or two ago by just eating a little more steak and some bagels? He said that they lose too many patients, because women don’t want to be told to gain or lose weight. I basically told him I thought this was ridiculous, and he kind of agreed.
So this is just a long-winded response to your observation that you were never told to gain weight or modify your exercise routine, it is frustrating when the simple solutions are brushed aside in favour of more invasive methods. On the bright side, I’m just a few weeks behind you — 20 weeks now!
Loved your post, Sarah!! As yet another person who has dealt with HA for 10 plus years, I strongly urge anyone reading this who suffers from amenorrhea to have a doctor check for thyroid and other issues….and if nothing is found, you really may need to evaluate your weight and activity level. I had HA for years with a BMI of 23-25, so don’t count yourself out just because you are in a "healthy BMI" range. In order to get pregnant (both times!), I had to gain weight and stop exercising. It was hard since I was not thin to begin with. But oh is it worth it! Thanks for bringing awareness, Sarah.
I wish I’d had your blog to read when I was taking Endo of Reproduction last year. Big fan of your blog. 🙂
It’s also interesting to note that it’s necessary to have at least 17% body fat to start puberty in girls…but that if you lose your periods (hypothalamic amenorrhea) due to decreased body fat, the threshold is raised – 21% body fat – to re-start menstruation.
Great post! I am in this very situation right now and it helps to read this and understand more – Right now I have low estrogen and no LH surge as far as I know so about a month ago I started adding more healthy fats into my diet, taking Calcium pills, reduced my exercise, specifically cardio. i am hoping some brings back my friend soon 🙂 I have a BMI of 19, so need to gain a few lbs (which is kinda scary I admit) and I am not sure on my body fat %. I ran my first marathon back in May and am sure this is a result from my training. But thank you again 🙂
I lost my period for 6 months, I think from stress (it’s back now, but still irregular). When I was given provera after 4 months with no period, I barely, barely spotted. I didn’t get a period until I went on antidepressants to help with my anxiety disorder. This sounds like hypothalamic amenorrhea to me, but I don’t know—can women with HA bleed from provera?
A strong and healthy physical body could positively have an effect on self-confidence, psychological vigor and emphasis. Physical recuperation could be affected by an individual’s belief and resolution. A negative attitude or perspective can drain an individual’s durability and power. Dealing with our physical bodies is an obstacle and also an advantage. Following I will certainly share the many portals which I am Thankful for … A Fit and Healthy Physical body.
OM Workout provides the most useful fitness tips and exercises for people who need it.
manage blood sugar with exercise
I have been following this plan for a few weeks now. I am amazed at the differences that have been showing in that time. I have dropped 8lbs and a pants and shirt size. I do the cardio every day except when I am doing lower days. In those 3 weeks, I took one cardio day off to let the legs heal up and bit from too much pushing and back at it again. Have restricted my diet to about 1300 calories a day. Thanks for posting this plan. Its really helping!medical weight loss nyc
I had optional amenorrhea and didn’t get my period for over a year. After many tests, precluding PCOS, hypothyroidism, and so forth., I wound up utilizing progesterone difficulties to kick off things…I likewise chop path down on my running, began eating more fats lastly, my cycle returned to ordinary. However, I’m panicked about the impact on my richness, so I value this clarification.